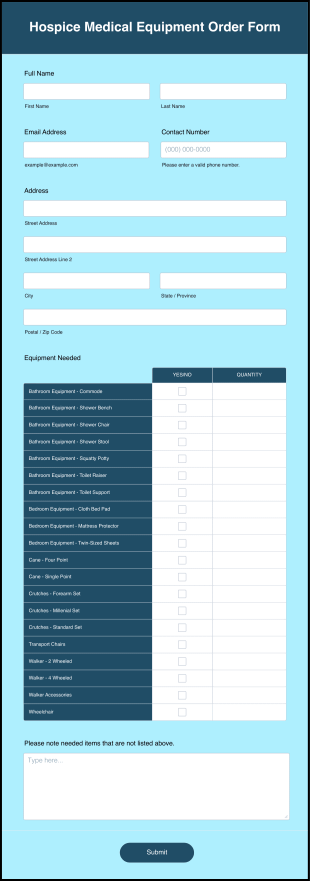
A Hospice Referral Form is a document used by the health care provider when referring a patient who is terminally ill to hospice care. This type of institution specializes in attending to the needs of these types of patients. The focus of care is a little bit different from other institutions because the patient in hospice care needs a different type of care like focusing on emotional, spiritual, and mental needs.
This Hospice Referral Form contains form fields that ask for the patient information, contact details, emergency contact details, and medical insurance number. This form template also checks the health status of the patient by asking for the medical diagnosis, allergies, and medications the patient is currently taking. It also has a referral date, referrer name, name of the institution, and reason for referral. This form template has a section for the health care provider and asks for the physician's name, contact details, and physician's signature. This form template can easily be modified via the Form Builder.